Lightning Bolts, Defibrillators, and Protection Circuitry Saves Lives
By Bill Laumeister, Strategic Applications Engineer, Maxim Integrated
Featured Products
Featured Manufacturers
Resources
Abstract: There have been many studies concerning the safe current levels impressed across the heart. The standards for medical equipment have bounced around, and today safe levels are said to be less than 4μA to 10µA. With lives in the balance, a designer of defibrillators must understand the entire gamut of possible input protection methods and then choose the best defense at a reasonable cost. Victims of sudden cardiac arrest (SCA) can be saved with a small, prompt lightning bolt (defibrillator shock) to the chest.
With lives at stake, the design of medical equipment is very demanding with extremely tight margins. Remember too that it is not uncommon to have several pieces of equipment attached to the patient at the same time. So the total leakage current must remain below the threshold that can harm the patient’s heart. This app note discusses several ECG input protection methods including radio susceptibility (RFI), ESD, electromagnetic interference (EMI), electromagnetic susceptibility (EMS), and defibrillator protection.
A similar version of this article appeared July 2014 in Electronic Design.
Introduction
Victims of sudden cardiac arrest (SCA) can be saved with a small, prompt lightning bolt (i.e., a defibrillator shock) to the chest. The shock (3kV to 5kV and 50A) stops the heart from unproductive fluttering (fibrillating) which fails to pump blood to the brain and other organs. This lightning bolt allows the heart to restart orderly pumping of blood. In hospitals it is common to monitor the heart using an electrocardiograph (ECG) with a separate defibrillator. The ECG leads (i.e., electrodes) are on the patient when the defibrillator delivers the shock. With no warning, the ECG must withstand this lightning bolt and continue working properly.
According to the American Heart Association (AHA) nearly 383,000 out-of-hospital sudden cardiac arrests occur annually, and 88 percent of cardiac arrests occur at home. Sadly, less than eight percent of people who suffer cardiac arrest outside the hospital survive [1]. These are sobering statistics. In medical terms a heart attack is much different than an SCA. An SCA has no warning signs; a person just collapses. A heart attack has multiple, generally understood warning signs preceding it.
Without our protective skin a patient’s heart is vulnerable to very small currents. In the electrically susceptible patient, moreover, even minute amounts of current (10µA) can cause ventricular fibrillation [2]. Remember that with an ECG and separate defibrillator it is not uncommon to have several pieces of equipment attached to the patient at the same time. Clearly, the total leakage current must remain below the threshold that can harm a human heart.
Defibrillators and Life-Saving Shocks
Many think that a defibrillator restarts the heart, but actuality it stops the heart. There is a random beating in the heart called fibrillation, which means the heart is not coordinated and not pumping blood. The defibrillator shocks the heart into inactivity, allowing the normal sinus rhythm to restart.
Figure 1 shows a hospital-style defibrillator and a trained medical technician delivering a life-saving shock for milliseconds. The 3kV to 5kV voltage and 50A current are necessary to penetrate the chest and shock the heart. High voltage and current is necessary because the human body is ˜75% salty water. The body conducts the majority of the electricity away, bypassing the heart.

Figure 1: A hospital-style defibrillator with paddles. Note that there is an external electrocardiograph (ECG) or heart monitor on the patient, as evidenced by the white circles (electrodes) and leads (wires) on the chest.
A second type of defibrillator (Figure 2) is an automated external defibrillator (AED) designed to be used by a member of the public with minimum training. These disposable electrode patches serve two purposes: first, monitor the heart with an electrocardiograph (ECG); and second, apply the high-voltage shock.
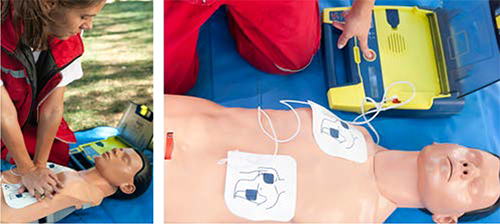
Figure 2: Chest compression CPR circulates blood to deliver oxygen to the brain and other vital organs until the heart can be restarted by the AED (right).
The AED protects its own input from the high voltage and current shock because it knows when it is about to apply the shock. Therefore it can, and does, disconnect the ECG monitor during the shock. The hospital-style defibrillator, however, is often used with a separate ECG or monitor. In this latter situation the ECG or monitor has no advanced warning and must withstand the high-voltage and current of the shock.
Protecting the Defibrillator for ECGs
We learned in Figure 1 that the voltage might be 3kV to 5 kV at 50A. The defibrillator test set in Figure 3 looks very much like the standard ESD test set4. There is, however, an important difference. The ESD test has a capacitor measured in picofarads, but the defibrillator test set is in many microfarads. The extra energy from the defibrillator must, therefore, be dissipated in front of the ECG.